A 5-point Unification Hypothesis for PANS & PANDAS
26th October 2024
In 1979 the Boomtown rats released a single, “I don’t like Mondays”, the background to the song is tragic and were the words used by a shooter in San Diego to explain her actions. After a request from Steve Jobs to play at a gig, Bob Geldof was inspired to write the first line of the song, “The silicon chip inside her head was set to overload”. It is timely that in 2024, Apple launched its new range of iMac computers which contain a silicon chip. This is whilst we work out the mechanism of action of the brain dysregulation in patients with PANS PANDAS. The claustrum, a paper-thin region in the brain next to the basal ganglia, takes on a role aligned with a silicon chip and I propose that it is the impaired activity of this area that then leads to many of the symptoms that we see in this group of patients. So, let’s try and untangle this theory.
The unification hypothesis has five parts:
1. Genetic predisposition
2.history of Group A Streptococcus Infection
3. Breakdown of the blood brain barrier
4. Inactivation of cholinergic interneurons
5. Claustrum dysregulation
Genetic predisposition
Our experience in the London PANS Clinic and The Children’s e-Hospital is that when we diagnose patients with PANS PANDAS, we quite often find other members of the family affected with similar symptoms, sometimes in the past when they were younger, but often with other siblings. This begs the question of whether, there is a genetic predisposition, and the fact that more than one member of family is commonly affected, does suggest an underlying genetic predisposition. This predisposition is, however, about the relationship of an individual’s genotype with the structure of Group A Streptococcus. And what I mean by this is that we know that molecular mimicry is a key component in the pathogenesis of PANDAS (1, 2) i.e. that the antibodies that are generated in response to a Group A Streptococcal infection, have, in a PANS PANDAS patient, an affinity with proteins on the cell surface in the brain, which is considered to be the mechanism by which neuroinflammation occurs in these patients, resulting in neuropsychiatric symptoms such as OCD, tics and anxiety. Put in very simple terms, these antibodies somehow gain access to cells in the brain and perform a type of molecular tickle. However, to do this, there would have to be a breakdown of the blood brain barrier which normally provides protection for the brain from insults such as antibodies and chemicals. This genetic predisposition should also be viewed in a more dynamic way, rather than the rigid protein antibody receptor mechanisms that are often postulated, and this is because streptococcus evolves, and everybody has a slightly different genetic make-up and therefore it’s the relationship between that genetic profile of the individual and the structure of the Group A Streptococcus In question that is important to consider. This relationship between the antibody and the receptor on the cells in the brain is likely to be unique to each individual and the subsequent receptor – antibody interaction will influence the clinical picture.
A history of Group A Streptococcus infection
Most people get their first strep throat infection in early childhood, typically between the ages of 5 and 15. Strep throat, caused by Streptococcus pyogenes (group A Streptococcus), is highly contagious and often spreads in close-contact settings, like schools or daycare. Younger children, especially those in elementary school, are particularly susceptible due to increased exposure to others who might carry the bacteria.
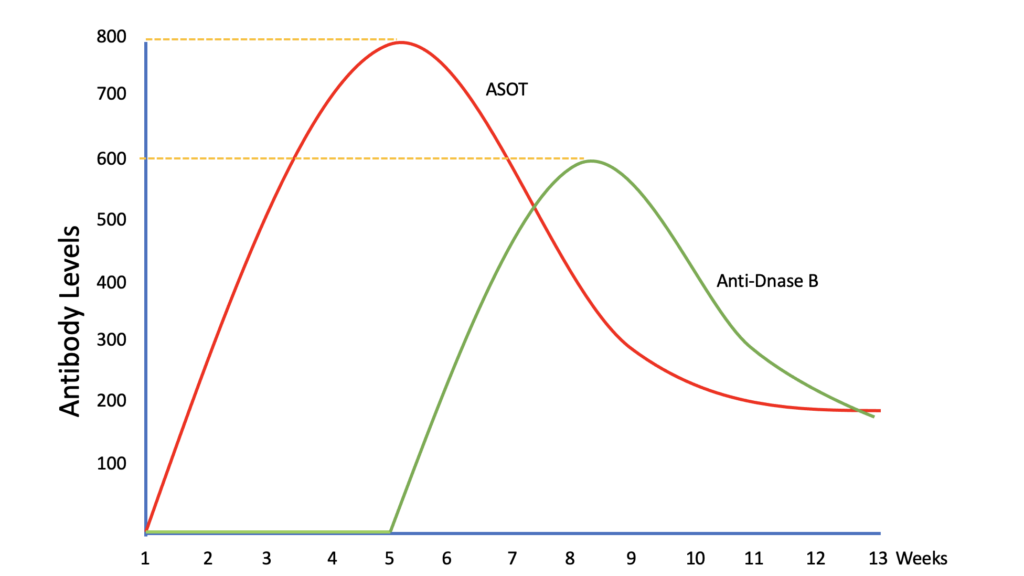
Although strep throat is less common in adults, they can still get it, especially those who work with children or are parents of young kids. Infections can occur year-round, but strep throat cases peak in late fall, winter, and early spring, when people tend to gather indoors. The graph below shows the normal pattern of antibody production following a first Group A Streptococcus infection.
Thus, after the first infection, the antibodies rise and then fall but they do not fall to zero. This is the basis of immunity. The point here is that there are always antibodies present after resolution of the initial infection, even though those antibodies might be present at low levels.
Breakdown of the blood brain barrier
How do these antibodies get through the blood brain barrier? That question appears to have been answered by a combination of workers including Spalice in Rome (3) who reported a trend toward higher TNF-alpha and IL-17 levels, and lower C3 levels in PANDAS patients compared to a control group. These cytokines along with Il-1beta can cause a rise in enzymes that can degrade the integrity of the blood brain barrier. Mondal, at this years inflammatory brain disorders conference (4) presented evidence to suggest that cytokines play a key role in the upregulation of matrix metalloproteinase 9 (MMP-9) which in turn results in the breakdown of the blood brain barrier in the area around the basal ganglia specifically. It is this breakdown in the integrity of the blood brain barrier that allows the antibodies to cause neuroinflammation. This is important as it may shift how we approach treating these patients and it would also explain the role of secondary infections such as Covid and chicken pox in increasing PANS PANDAS symptoms by increasing MMP-9 and breaking down the blood brain barrier even in the absence of an active group A streptococcal infection, by giving the pathogenic antibodies access to the brain. This brings together the pathways for PANS and PANDAS.
Inactivation of cholinergic interneurons
Xu & Pittenger have published data on the presence of antibodies in children with PANDAS that bind to and specifically inhibit cholinergic interneurons (CINs) in the basal ganglia (5, 6).
IgG antibodies from PANS cases showed elevated binding to striatal CINs in both mouse and human brain. “Patient plasma collected during symptom flare decreased a molecular marker of CIN activity, phospho-riboprotein S6, in ex vivo brain slices; control plasma did not. Neither elevated antibody binding to CINs nor diminished CIN activity was seen with plasma collected from the same children during remission. These findings support the hypothesis that at least a subset of PANS cases have a neuroimmune pathogenesis. Given the critical role of CINs in modulating basal ganglia function, these findings confirm striatal CINs as a locus of interest in the pathophysiology of both PANS and PANDAS”

The Claustrum
The claustrum is a long and irregular sheet of neurons nestled between the insula and striatum. As it is known to be heavily and bilaterally connected to many brain regions in organisms ranging from mice to humans. It is paper thin but considered by many as the conductor of brain activity in the same way that a conductor leads an orchestra. It has an input and output function and is therefore easily related to the function of a computer processor or silicon chip.(7) The claustrum may also have an important role in learning (8) and it must be remembered that the aberrant messages that the claustrum may receive following the PANS PANDAS process will not have any learning associated with it and it is therefore not surprising that this leads to anxiety and or phenomenon. We should also consider the role of the insula that connects with the claustrum and which has a role in modulating sensory input to the claustrum (9). Misophonia, visual disturbances (such as word wobble) and urinary symptoms are common in our PANS PANDAS population. If we accept the role of the claustrum as being one of processing and conducting brain activity and actions, we can see that anything that impairs the processing ability of the claustrum will result in the impairment of the processing of sensory stimuli from the insula(10). The question is, does this happen? The striatum and the claustrum are both involved in integrative processing, but they interact indirectly rather than through direct, well-defined pathways. These include cortical projections, thalamic connections, basal forebrain cholinergic systems and functional connectivity. Neuroimaging studies have revealed functional connectivity between the claustrum and basal ganglia circuits, including the striatum. While these connections aren’t anatomical pathways, they indicate synchronized activity patterns that suggest the two regions work together, likely in processing complex behaviours such as sensorimotor integration and attentional control.
In 2005, Crick and Koch published a paper on the function of the claustrum, unfortunately Crick died before the paper was completed but it provides a powerful argument for the role of the claustrum as described (11). It describes the claustrum as the “seat of consciousness” and even suggests that it is from this epicentre that seizures arise.
Summary
I propose a five-point hypothesis that suggests that in patients who have the correct genetic and environmental predisposition, antibodies are produced that cross react with the basal ganglia. This occurs following breakdown of the blood brain barrier which is mediated by cytokines produced in response to infection and inflammation. These antibodies inactivate cholinergic interneurons in the basal ganglia which results in a disturbance in the function of the striatal-claustrum axis. Put together, these combine to produce the symptoms commonly seen in patients with PANS & PANDAS. Importantly, this hypothesis would align the pathological mechanisms underpinning both PANS and PANDAS.
Dr Tim Ubhi
26th October 2024.
References
- Kirvan CA, Swedo SE, Kurahara D, Cunningham MW. Streptococcal mimicry and antibody-mediated cell signaling in the pathogenesis of Sydenham’s chorea. Autoimmunity. 2006;39(1):21-9.
- Swedo SE, Leonard HL, Garvey M, Mittleman B, Allen AJ, Perlmutter S, et al. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections: clinical description of the first 50 cases. Am J Psychiatry. 1998.
- Leonardi L, Lorenzetti G, Carsetti R, Piano Mortari E, Guido CA, Zicari AM, et al. Immunological characterization of an Italian PANDAS cohort. Frontiers in pediatrics. 2023;11:1216282.
- Mondal A. PANS Plasma Effects on the Blood-Brain Barrier. Inflammatory Brain Disorders Conference 20242024.
- Xu J, Liu RJ, Fahey S, Frick L, Leckman J, Vaccarino F, et al. Antibodies From Children With PANDAS Bind Specifically to Striatal Cholinergic Interneurons and Alter Their Activity. Am J Psychiatry. [Research Support, N.I.H., Extramural Research Support, N.I.H., Intramural]. 2021 Jan 1;178(1):48-64.
- Xu J, Frankovich J, Liu RJ, Thienemann M, Silverman M, Farhadian B, et al. Elevated antibody binding to striatal cholinergic interneurons in patients with pediatric acute-onset neuropsychiatric syndrome. Brain, behavior, and immunity. 2024 Jul 29.
- Wong KLL, Nair A, Augustine GJ. Changing the Cortical Conductor’s Tempo: Neuromodulation of the Claustrum. Frontiers in Neural Circuits. 2021;15.
- Kim T, Capps RA, Hamade KC, Barnett WH, Todorov DI, Latash EM, et al. The Functional Role of Striatal Cholinergic Interneurons in Reinforcement Learning From Computational Perspective. Frontiers in neural circuits. [Research Support, Non-U.S. Gov’t]. 2019;13:10.
- Molnar-Szakacs I, Uddin LQ. Anterior insula as a gatekeeper of executive control. Neurosci Biobehav Rev. [Review]. 2022 Aug;139:104736.
- Kumar S, Tansley-Hancock O, Sedley W, Winston JS, Callaghan MF, Allen M, et al. The Brain Basis for Misophonia. Current biology : CB. 2017 Feb 20;27(4):527-33.
- Crick FC, Koch C. What is the function of the claustrum? Philosophical transactions of the Royal Society of London Series B, Biological sciences. [Review]. 2005 Jun 29;360(1458):1271-9.
Posted in: Dr Tim's Opinion, PANDAS by Dr Tim Ubhi



Comments
John Hewertson
2026-05-26 13:38:14
Which specific antibodies have been identified which cross react with the basal ganglia, and what sort of titres are required in the CSF to be of significance.
saliviqdiagnostics
2025-06-25 06:40:49
SaliviQ Diagnostics offers innovative saliva-based molecular diagnostics for strep throat and other infections. Non-invasive, accurate, and fast point-of-care PCR testing. Explore our saliva-based molecular diagnostic solutions for strep throat and other infections. Discover the benefits of non-invasive qPCR saliva tests.